Medical Guide
Pseudofolliculitis Barbae: How to Stop It For Good
Pseudofolliculitis barbae (PFB) is chronic ingrown hairs in shaved areas. Learn diagnosis, the three tiers of treatment, and how to prevent permanent scarring.
Pseudofolliculitis barbae (PFB) is chronic ingrown hairs in shaved areas. Learn diagnosis, the three tiers of treatment, and how to prevent permanent scarring.
This page contains affiliate links. We earn a small commission on purchases at no extra cost to you. This never influences our recommendations.
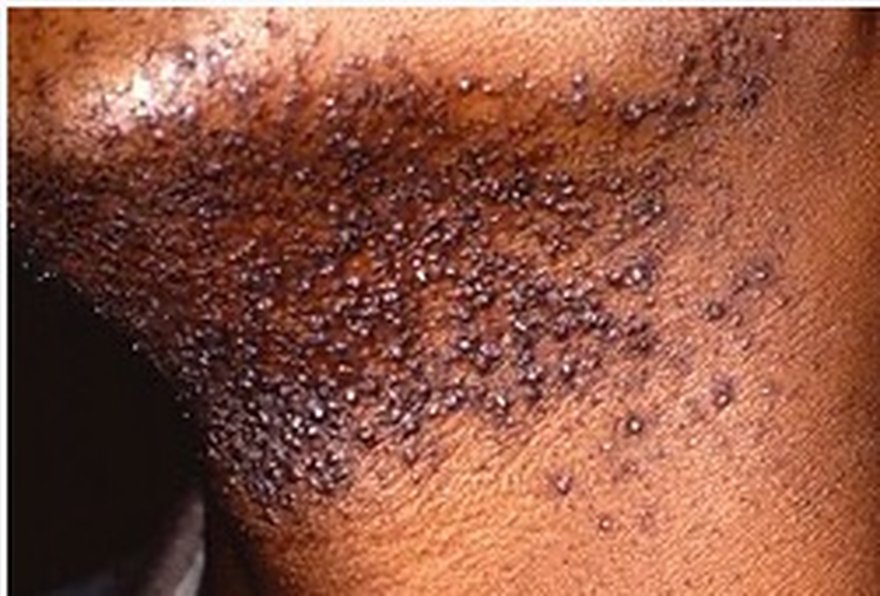
Pseudofolliculitis barbae (PFB) is the medical name for chronic ingrown hairs in shaved areas — most commonly the beard and neck, but also the bikini line, underarms, and chest. The Latin literally translates to "false inflammation of the beard hair follicle," reflecting that the bumps look like infected follicles but are actually caused by hair re-entering the skin. PFB shows up identically in the groin and inner thigh, where the thinner skin and constant friction make the same mechanism more visible and slower to clear.
PFB affects an estimated 60% of Black men, 30% of Latino men, and 10-15% of white men who shave their faces regularly. The condition is also common in women who shave or wax the bikini line and underarms. The defining factor is curly or coiled hair: as the hair grows back after cutting, it curves and re-enters the follicle wall or the skin surface beside the follicle. PFB on the chest and back follows the identical mechanism in men who wax, sugar, or shave these areas — the only difference is surface area.
PFB is technically a chronic skin condition, not a cosmetic problem. In its more severe forms it can cause permanent scarring, dark spots (post-inflammatory hyperpigmentation), and keloid formation. Early and consistent management is critical.
PFB presents as recurring papules and pustules in shaved areas. The clinical pattern:
The PIH that follows pseudofolliculitis barbae has its own treatment ladder. Here's what works.
The science of follicle scarring and the tiered treatment approach for chronic spots that won't resolve.
A dermatologist will diagnose PFB clinically based on this pattern. Bacterial cultures are typically negative, distinguishing it from true folliculitis (bacterial follicle infection) which requires antibiotics. When papules and pustules appear in clusters of ingrown hairs rather than scattered individually, PFB is the most likely underlying cause.
| Feature | PFB | Bacterial Folliculitis |
|---|---|---|
| Cause | Curly hair re-entering skin | Bacterial infection (often Staph) |
| Trigger | Shaving, waxing, plucking | Sweat, friction, broken skin |
| Pus | Sterile (no bacteria) | Active infection |
| Cultures | Negative | Positive for bacteria |
| Treatment | Hair removal modification, exfoliation | Topical or oral antibiotics |
| Spread | Does not spread | Can spread between follicles |
Confusion between the two leads to inappropriate antibiotic use, which doesn't address the underlying mechanical problem of PFB.
For mild-to-moderate PFB, the standard first-line approach combines:
This combination resolves 60-70% of mild PFB cases within 4-6 weeks of consistent use.
Combines salicylic and glycolic acids in a single formula — addressing both the active and preventive sides of PFB. Apply twice daily after shaving. Fragrance-free for sensitive post-shave skin.
If topical treatment alone is insufficient, the next step is changing how you remove hair:
For severe or treatment-resistant PFB, laser hair removal is the definitive solution. After 4-8 sessions, hair density is permanently reduced enough to eliminate PFB. Long-pulse Nd:YAG laser is the preferred wavelength for darker skin tones.
For complete information, see our laser hair removal guide.
Once PFB is under control, prevention requires ongoing maintenance. The minimum effective protocol:
Prescription-strength treatments available through a dermatologist include topical retinoids (tretinoin), eflornithine cream (slows hair regrowth), and oral antibiotics if true folliculitis develops on top of PFB.
New product reviews, ingredient breakdowns, and dermatologist Q&As.
Free monthly newsletter. Unsubscribe anytime.
Get expert tips, new product reviews, and dermatologist Q&As. Free, every month.